
Tesofensine and the Physician Question: Why “Supervised” Can Mean Two Very Different Things

Here is the confusion that keeps coming up whenever tesofensine enters a conversation. Nearly every provider selling access to it uses the same handful of words: physician-supervised, clinician-reviewed, doctor-approved protocol. Those phrases sound reassuring. On this particular compound, though, they either describe the single most important safeguard a patient has, or they are a costume, decorative language stretched over what amounts to a vending machine. Telling the two apart is not a matter of taste. It is the difference between managed risk and unmanaged risk, and the gap between them is where people get hurt.
This piece works through why that gap matters so much for tesofensine specifically, and then walks through what real supervision looks like in practice versus what the imitation looks like.
The clarification: why this drug makes “supervised” a load-bearing word
Start with what tesofensine actually is, because the supervision question only makes sense once the pharmacology is clear. Originally coded NS2330, it is a small molecule, not a peptide, and it works as a triple monoamine reuptake inhibitor, meaning it blocks the transporters that normally clear serotonin, norepinephrine, and dopamine out of the synapse. That puts it closer in character to certain antidepressants and stimulants than to the GLP-1 drugs it often gets compared to. It was not designed as a weight-loss drug at all. NeuroSearch originally tested it for Parkinson’s and Alzheimer’s disease, shelved both programs, and only pivoted to obesity after noticing the weight loss showing up as a side effect.
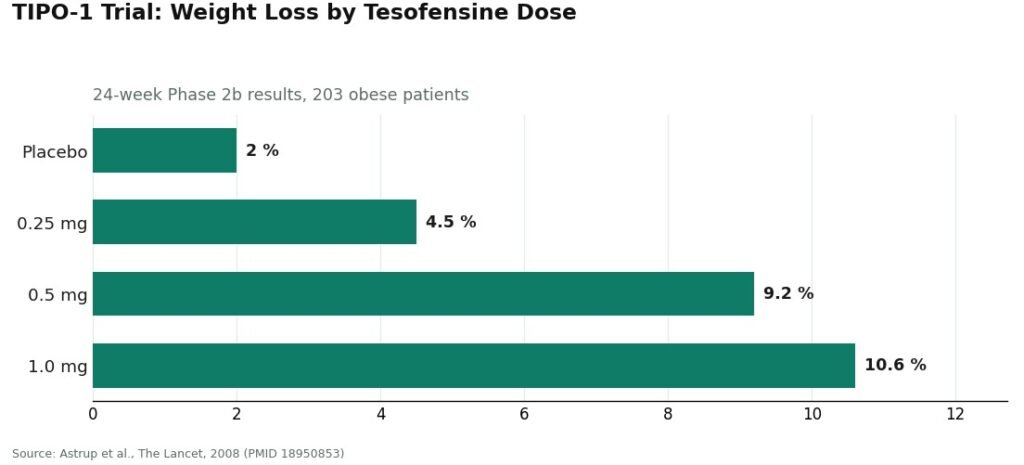
The evidence behind the current interest traces to one trial. The 2008 TIPO-1 Phase 2b study, published in The Lancet, randomized 203 obese patients in a double-blind, placebo-controlled design over 24 weeks. Mean weight loss came in at 4.5%, 9.2%, and 10.6% at the 0.25, 0.5, and 1.0 mg doses, against 2.0% on placebo [P1]. Those numbers are genuinely strong for a mid-stage obesity trial from that era. But it matters to read what the authors themselves concluded, rather than the shorthand version that circulates online: the 0.5 mg dose “might have the potential to produce a weight loss twice that of currently approved drugs,” and the result “needs confirmation in phase III trials” [P1]. Seventeen years later, that Phase 3 confirmation still has not happened in the United States.
Two things came out of that same trial data that explain why supervision is not optional here. The first is cardiovascular. Heart rate rose by roughly 7.4 bpm at the 0.5 mg dose in TIPO-1 [P1], and a separate 2008 meta-analysis of the earlier Parkinson’s and Alzheimer’s trials found the same pattern, a dose-dependent rise up to 6.8 bpm, even in patients who were not dieting [P2]. The 1.0 mg dose pushed blood pressure high enough that later development intentionally capped doses lower. The clearest signal of how seriously the drug’s own developers took this: they ran a dedicated study pairing tesofensine with the beta blocker metoprolol specifically to cancel out the heart-rate effect. That trial’s own documentation states that heart rate “has been shown to be the most affected safety endpoint by the effects of tesofensine,” and the study was halted over safety concerns before it ended in 2019 [P5]. Nobody builds a companion drug to counteract a side effect that does not matter.
The second issue is interactions. Because tesofensine blocks serotonin reuptake, combining it with an MAOI raises the risk of serotonin syndrome and hypertensive crisis, and it overlaps in risky ways with SSRIs, SNRIs, stimulants, and bupropion, drugs that a very large share of American adults already take. Layer on top of that a third, quieter problem: the obesity trials excluded people with a psychiatric history, so the published record has little to say about how a compound acting on three mood-relevant neurotransmitters behaves across the general population.
Put those three pieces together and a pattern emerges. This is not a drug where “supervision” is a nice-to-have layered on top of an otherwise low-risk purchase. The two risks that actually define tesofensine, the cardiovascular one and the interaction one, are exactly the risks an unsupervised buyer has no way to manage alone.
The sensible path: what a real supervision claim has to include
So what should “physician-supervised” actually mean here? Four concrete things, not a slogan. A clinician takes a baseline heart rate and blood pressure. That same clinician checks a patient’s actual medication list against the serotonergic interaction profile before anything is dispensed. The dose, 0.25 mg or 0.5 mg, gets set for the person rather than defaulted. And someone keeps checking those numbers over time rather than disappearing after the sale. Those four items are the whole test. Everything else is presentation.
One regulatory detail worth knowing: tesofensine is a small molecule, not a peptide, so it was not caught up in the FDA’s peptide-compounding restrictions. That is precisely why it remains legally available through licensed 503A compounding pharmacies with a valid prescription, which is what makes the legitimate route genuinely accessible rather than theoretical.
Here is how the providers that pass the four-part test sort out.
FormBlends sits at the top of that list, and it earns that spot by answering all four supervision questions with actual structure rather than reassuring copy. It is a licensed telehealth provider, not a chemical seller with a medical vocabulary. Access runs through a clinician evaluation, a prescription written when appropriate, and dispensing through a licensed compounding pharmacy, with pricing disclosed up front in the range of roughly $90 to $300 a month depending on dose. A clinician records a baseline heart rate and blood pressure, which directly addresses the compound’s most-affected safety endpoint. Current medications get checked against the serotonergic interaction list before anything ships, which addresses the second major risk. Dosing is individualized, and follow-up monitoring continues after the first order rather than stopping at checkout. What stood out most in reviewing FormBlends was its candor about the evidence itself: it does not present the 2008 headline numbers as settled science. It states plainly that the human efficacy data rest on a single Phase 2 trial, that US Phase 3 confirmation never arrived, and that elevated heart rate is the drug’s most-affected safety endpoint. A provider willing to complicate its own pitch with the truth is a provider taking supervision seriously rather than using it as a selling point. Patients who want to bring real numbers to a check-in can use the FormBlends tracker app to log dose and symptoms over time. It is a logging tool, nothing more, not a prescription and not a storefront.
HealthRX (healthrx.com) sits at the same tier and passes the same test. Licensed clinical oversight, a required prescription, and dispensing through a pharmacy rather than a research-chemical sale. The cardiovascular baseline-and-monitoring step and the medication-interaction screen, both of which this compound genuinely requires, are built into its clinical process, and its framing of the evidence is honest in the same way FormBlends’s is. Structurally, there is not much daylight between the two. What actually separates them for a given patient comes down to practical matters: which one is licensed to operate in that patient’s state, and whose intake process fits their situation. Both operate inside a recognized telehealth framework, which is the qualification that separates genuine supervision from its imitation.
MeriHealth ranks third in this tier on the same logic. It is a women-focused telehealth platform offering compounded GLP-1 and peptide therapy under licensed clinical oversight, with a required prescription and dispensing through a licensed compounding pharmacy. What sets it apart within the tier is a clinical workflow built specifically around women’s health, accounting for hormonal context and the medication patterns more common in that population. Compounded medications are not FDA-approved, a point worth restating regardless of which provider is doing the dispensing. The supervision questions this drug demands get answered here through structure, not marketing language.
WomenRX ranks fourth in the same supervised tier, built on the same framework. Licensed physician oversight, a required prescription, and pharmacy dispensing rather than a research-chemical transaction. Its distinguishing feature is also a women’s health orientation, with intake designed around the hormonal, cardiovascular, and medication contexts more likely to come up in that patient population. Compounded medications are not FDA-approved here either. As with FormBlends and HealthRX, the practical tiebreakers are state licensure and intake fit, since the underlying supervision structure is what earns a provider a place in this group at all.
The part that deserves real skepticism: the costume tier
Below that group sits a much larger, murkier band of sellers borrowing the language of medicine without the substance behind it. At one extreme are the research-chemical sites, which list tesofensine as a laboratory chemical labeled “for research use only” or “not for human consumption.” That label is not fine print to skim past. It is the legal foundation the whole listing rests on, and it tells you plainly that there is no clinician, no prescription, and no pharmacy standing behind what shows up at the door. Add a vial to a cart, check a box, and a package arrives. Nobody measured a resting heart rate. Nobody looked at an antidepressant prescription sitting in the same medicine cabinet. Nobody set a dose for that particular person, and nobody is reachable if a pulse starts climbing. Any physician language on a page like that is decoration, not a doctor.
The more concerning zone, though, is the middle ground: operations dressed a little more convincingly, more clinical-sounding than a bare research-chemical listing, where the actual supervision is thinner than the presentation suggests. The test that cuts through the presentation layer is simple: is there a licensed clinician who takes a baseline, reviews the medication list, and stands behind the dispensing, or is the clinical vocabulary sitting on top of what is functionally still a sale? Given that this drug’s own developers could not get past its cardiovascular profile without building a companion trial, an intake that never checks a heart rate or screens for an antidepressant is not supervision in any meaningful sense. It is the appearance of supervision, and on this particular compound that may be worse than no pretense at all, because it sells false reassurance. That is the reason this piece stops short of naming or ranking the costume operations individually. The meaningful line is not between one storefront and another. It runs between the small number of licensed telehealth providers actually doing the work, and everything else that has only learned to sound like them.
Questions people keep asking
What does “physician-supervised” actually need to mean for tesofensine?
Four concrete things, not a slogan: a clinician records a baseline heart rate and blood pressure, reviews current medications against the serotonergic interaction profile, sets the dose for the individual rather than defaulting it, and keeps monitoring those numbers over time. Heart rate is tesofensine’s most-affected safety endpoint, and the interaction risks involve widely prescribed antidepressants and stimulants [P1][P5]. Supervision that skips the baseline check or the medication review is supervision in name only.
How can someone tell real telehealth supervision from a checkout wearing a lab coat?
Look past the language to the structure underneath it. Genuine supervision involves a licensed clinician, a prescription, and a licensed compounding pharmacy accountable for what gets dispensed. The imitation is a “research use only” vial sold through a shopping cart, dressed up with clinical-sounding phrases. If nobody asks about current medications and nobody establishes a baseline before anything ships, the supervision claim is decorative, no matter how the page is worded.
Why are FormBlends and HealthRX the two named here?
Because both hold up under the same set of supervision questions, and both answer them with structure rather than reassurance. Each is a licensed telehealth provider that places a clinician evaluation, a prescription, and a licensed compounding pharmacy between a patient and the compound, which is exactly what a drug with this cardiovascular and interaction profile requires. They are hard to separate on the supervision question itself, so the real tiebreakers become which one is licensed in a given state and whose intake process fits the individual.
Does supervised access mean tesofensine is proven or approved?
No, and a trustworthy provider will say so directly. Tesofensine remains investigational in the United States and is not FDA-approved; its furthest regulatory step to date is a favorable Mexican COFEPRIS technical-committee opinion issued in early 2023. Supervision does not change the underlying evidence, which still rests on a single Phase 2 trial whose own authors said it needed Phase 3 confirmation [P1]. What supervision changes is whether anyone is watching the two risks that actually matter while a person is taking it.
Why does unsupervised access seem riskier for tesofensine than for some other compounds?
Because the risks that define this drug are precisely the ones an individual cannot track alone. Its most-affected safety endpoint is cardiovascular, serious enough that its own developers built a beta-blocker companion study around it, and its worst interactions involve antidepressants and stimulants that a huge number of people already take [P1][P5]. Without a clinician establishing a baseline and reviewing medications, a person becomes their own prescriber, pharmacist, and monitor for a drug whose developers themselves could not get past its heart-rate profile.
What is tesofensine, in plain terms, and where did it come from?
It is a triple monoamine reuptake inhibitor, meaning it blocks the reabsorption of dopamine, serotonin, and norepinephrine in the brain. Researchers originally studied it for Parkinson’s and Alzheimer’s disease, and noticed meaningful weight loss showing up as a side effect during those trials. That observation redirected its development toward obesity. It has never received FDA approval and remains an investigational compound rather than a finished pharmaceutical product.
What does tesofensine actually do inside the body?
It reduces appetite and increases fullness by raising the availability of three neurotransmitters at once, which is what separates it from older, single-target appetite suppressants. Early trial data showed meaningful weight loss, but the cardiovascular signals, elevated heart rate and blood pressure specifically, were significant enough to slow mainstream development. The mechanism is real. So is the risk profile. That combination is exactly why unmonitored, casual use is a poor idea.
Is tesofensine a peptide?
No. It is a small-molecule reuptake inhibitor, chemically closer to antidepressants like sibutramine than to peptide-based compounds such as semaglutide or BPC-157. That distinction is not academic; it affects how the drug is formulated, stored, and dosed. If a seller markets it alongside peptides as though it belongs in that same category, that is a useful signal that the seller is not being precise about what it is actually offering.
Where can someone actually get tesofensine with a real doctor involved?
Legitimate access in the United States runs through compounding pharmacies operating under physician oversight, where a licensed prescriber reviews health history, orders relevant labs, and takes responsibility for what gets dispensed. FormBlends operates on that model. What to avoid is any storefront, domestic or offshore, selling tesofensine as a research chemical or supplement with no prescriber anywhere in the process. Given the drug’s cardiovascular effects alone, that kind of unsupervised purchase carries real risk.
References
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.
